When we hear the word “disease,” many examples may instantly come to mind. We primarily think of terminal illnesses such as cancer or infectious diseases such as HIV. Most people, however, are not as likely to think of alcoholism or addiction. Yet the disease model of addiction suggests that substance use disorder warrants such a classification. Learn how the disease model of addiction explains addiction and how it affects our understanding of substance abuse, and treatment approaches with this helpful guide from Avenues Recovery.
Key Takeaways on the Disease Model of Addiction
- The disease model of addiction views addiction as a chronic medical condition characterized by changes in brain structure rather than simply a failure of willpower.
- Addiction alters neural pathways, particularly those involving reward and self-control, leading to compulsive substance use despite harmful consequences.
- Environmental factors such as stress, trauma, social context, and exposure to substances interact with biological vulnerability, influencing both the development and progression of addiction within the disease framework.
- Critics argue that the disease model can downplay personal agency and neglect the significant roles of social, psychological, and cultural influences.
- The disease model shapes treatment approaches by emphasizing medical and therapeutic interventions similar to those of other chronic health conditions.
What Is the Disease Model of Addiction?
The disease model of addiction views addiction as a chronic, relapsing medical condition rather than a moral failing or lack of willpower. It is strongly supported by research in Neuroscience, which shows that repeated use of addictive substances or behaviors can alter brain structure and function, especially in areas responsible for decision-making and impulse control. These changes affect how the brain processes pleasure and motivation, making it difficult for individuals to stop despite harmful consequences. Under this model, addiction is similar to other long-term illnesses like Type 2 Diabetes or Hypertension, meaning it often requires ongoing treatment and support rather than a one-time cure.
When Was Addiction First Classified as a Disease?
The disease model has its roots in the 1849 essay "Alcoholismus Chronicus" by Swedish physician Magnus Huss, who looked into the disease theory of alcoholism. Some believe the disease model of addiction arose in recent decades as a ploy to eliminate the associated stigma of addiction, but this is incorrect.
In his essay, Huss described the defining characteristics of alcoholism, a term that did not exist prior to his use, as remarkably disease-like. Marked by systematic physical damage, this chronic disease often proves fatal. And much like cancer and some other fatal diseases, alcoholism and addiction sometimes go into a period of “remission” only to resurface later in the form of relapse.
Is Addiction a Disease? How the Disease Model Explains Addiction
Long after Huss wrote about alcoholism, several studies on alcohol and drug addiction backed up many of his claims. We now know that substance abuse does, in fact, change brain chemistry through a very systematic series of events.
Dopamine Surges
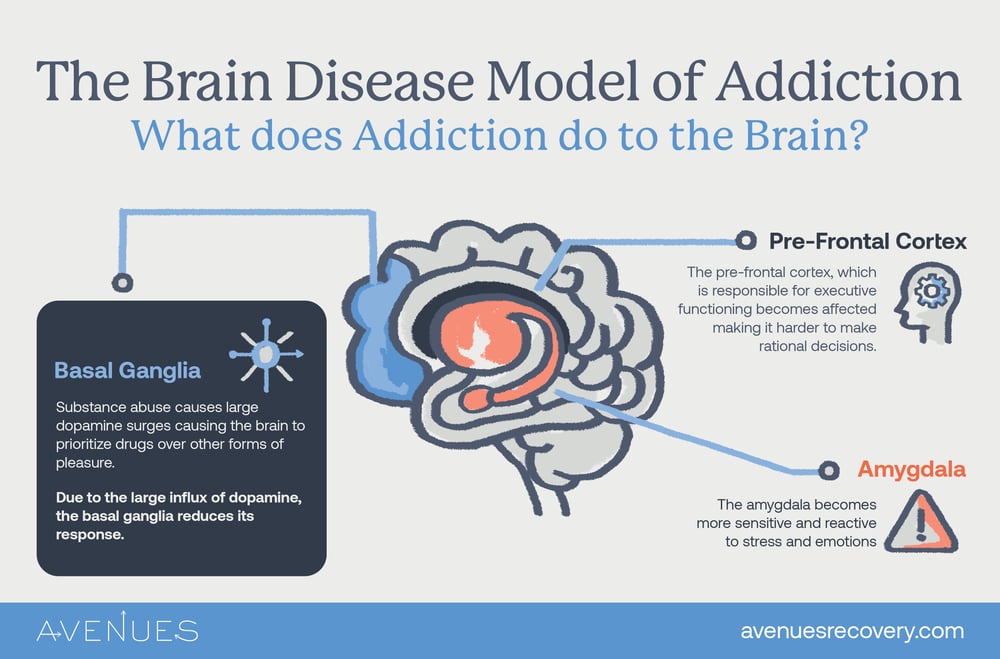
A strong influx of dopamine activates the brain’s pleasure circuits. This causes the user to feel increasingly intense urges to continue using. The National Institute on Drug Abuse (NIDA) explains that substances of abuse often release 2-10 times as much dopamine as normal behaviors, such as food or sex. As substance use provides such large surges of dopamine, the brain begins to prioritize the substance over other forms of pleasure, such as socializing or eating.
However, as the brain becomes accustomed to the excess dopamine, the basal ganglia, which is responsible for the “reward cycle,” reduces its response to it. This causes the user to need more of the substance to achieve the same high, locking them into a cycle, as described by the disease model of dependence.
Increased Stress and Strong Emotions
Repeated substance use causes the amygdala to become sensitive and reactive, especially to stress. This causes users to become more irritable and emotional, and gives them further reason to pursue substances as an escape from their feelings.
Impaired Executive Functioning
Addiction also affects the executive functioning part of the brain, causing users to struggle with their self-control and judgment. As the substance misuse increases, it becomes harder to make rational decisions. The prefrontal cortex, the area of the brain mainly responsible for executive functioning, is also the last section of the brain to fully develop, making teenagers particularly vulnerable to the effects of addiction.
Jellinek’s Stages of Addiction Development
The disease model of addiction treats chemical dependency as an illness that develops over time. As the dependent continues using, they develop increased tolerance. We often characterize tolerance in a model known as the Jellinek curve. This stems from biostatistician E.M. Jellinek’s work, The Disease Concept of Alcoholism, which breaks alcohol addiction into several stages.
Below is an outline of the different forms of alcoholism that occur and the different stages a user might find themselves at, as explained in “The Disease Concept of Alcoholism”.
- Alpha - Psychological dependence and emotional reliance begin in the alpha stage, when a user might turn to alcohol for relief or soothing. However, in this stage, the user can still control or limit the amount of alcohol he consumes.
- Beta - A beta alcoholic might find himself suffering from medical problems such as cirrhosis of the liver, but they are not physically or psychologically dependent.
- Gamma - By the time one reaches the gamma stage, they experience increased symptoms of tolerance. Gamma alcoholics are not in control of their drinking once they start.
- Delta - At the Delta stage, users are drinking to avoid withdrawal symptoms and are caught in the cycle of substance misuse. A Delta alcoholic may still be able to control what he consumes in each drinking session, though.
- Epsilon - The final stage is characterized by heavy binge drinking episodes where the user is not in control.
Though therapy is always helpful to someone struggling with addiction, once a user reaches the gamma stage of addiction, they are much more likely to need intensive outside support to be able to recover.
Environmental Factors and the Brain Disease Model of Addiction
There are many outside factors that play a role in how the disease model of addiction plays out. Some users are more susceptible than others to being caught in the cycle of disease once they start using. Despite this understanding, the initial use of a substance must still be based on some form of choice, and the disease model of addiction or genetics cannot be considered the sole reasons someone develops an addiction. Below are some factors that can contribute to the development of addiction.
- Genetics sometimes plays a role in the development of substance dependence. Heritability is generally considered to constitute about 50% of an individual’s risk of developing addictive tendencies, although the substance in question plays a large part in this. Alcohol addiction is much more likely to be hereditary than methamphetamine addiction.
- Military service or childhood trauma may also cause users to turn to substance abuse as a means of escaping PTSD or pain from adverse experiences.
- Peer pressure and volume of exposure can also push someone into addiction by making it more likely they will try the substance.
- Physical ailments may cause someone to develop an addiction as they are susceptible to the same flood of dopamine and increased tolerance when they use painkillers, even if escapism is not involved.
Facing Criticisms of the Disease Model

Despite the reasons of many medical professionals for adopting the disease model of addiction, criticisms still abound. Critics believe that the systemic effects on the body are insufficient to meet the definition of disease. They note the lack of certain pathological factors that characterize most diseases, or infectious cellular agents that would normally play a role in a disease’s spread throughout the body. Additionally, while the body certainly degenerates as a result of chronic substance abuse, critics note that addiction itself does not qualify as a biologically degenerative ailment.
Unfortunately, we rarely see these criticisms take the form of a discussion. Articles and studies address the addiction disease model, while opposing articles and studies offer choice as an academic counterblast. Regardless of whether we classify substance misuse as addiction or disease, it remains a debilitating psychological condition for which many require help. A primary benefit of the medical model of addiction is that it helps greatly in forming a consensus regarding the best forms of treatment, allowing us to better ensure a successful and effective entrance into recovery.
The Disease Model of Addiction in Treatment

Many treatment centers utilize the disease model of addiction. Its insights into the process through which addiction affects our bodies and minds prove highly beneficial.
For instance, the physical effects of addiction inform the detox process. In Jellinek’s stages of alcoholism, the greatest increases in tolerance occur after substance abuse has already begun to impact the user’s body. By this time, the brain and body have undergone massive changes. The result is that quitting often leads to withdrawal symptoms. It is not enough to keep detox patients in a safe space and prevent them from using drugs at a detox drug rehab. They must also receive medical treatment to ease their withdrawal.
We also know, due to the disease model, that addiction develops and worsens over time. This influences our treatment approach at Avenues Recovery. First, we get the client to a safe place where they can maintain abstinence, thereby halting the progression of the disease. Our medical support staff will then assess the client and provide any medications or other treatments required to address any physical degeneration they may have suffered. With these elements in place, our clinical staff helps the client formulate an individualized treatment plan that allows them to adjust their thinking and resist the urge to use.
Behavioral Interventions for Substance Misuse
The user’s thinking must also be taken into account when treating addiction. NIDA states that understanding how addiction affects brain processes has already resulted in several effective medicines, as well as new and promising medication targets to treat drug and alcohol addiction.
Behavioral interventions play an especially prominent role in addiction treatment services. In early sobriety, the desire to use lingers strongly. Even without physical cravings, the user remembers the rush of that dopamine surge. They may obsess over the thought of experiencing it again. At Avenues, we therefore devote significant effort to peer support and relapse prevention. The best recovery plan is one that allows the addict or alcoholic to pursue a fulfilling life - a life that will provide natural rewards once the previous source of dopamine is no longer available.
Treatment for Addiction Disease at Avenues
Avenues Recovery offers proven behavioral interventions in numerous forms. Our detox and rehab programs take the disease model of addiction into account, and our programs are tailored accordingly. These range from cognitive behavioral therapy and addiction education to faith-based programs and holistic care options. For more information on how we can help you to fight the disease of addiction, reach out to one of our experienced counselors. Start your journey to recovery today.
FAQs on the Disease Model of Addiction
How does addiction change the brain?
Addiction changes the brain by increasing dopamine release by 200–300% in reward circuits. Repeated use weakens prefrontal cortex control and strengthens habit pathways in the basal ganglia. These changes reduce impulse control, increase cravings, and make stopping use difficult over time.
Is the disease model of addiction outdated?
The disease model of addiction is not outdated but has evolved. Modern neuroscience shows addiction alters brain structure and function, especially in reward and control systems. Current models integrate disease, behavioral, and social factors.
Do 12-step programs use a disease model of addiction?
12-step programs use a disease model of addiction by defining addiction as a chronic, progressive condition with loss of control and lifelong risk of relapse. Programs like AA and NA emphasize abstinence and ongoing management. They also integrate spiritual principles and peer support alongside the disease framework.